
PATHOLOGIES








Hip Osteoarthritis or coxarthrosis
It is a gradual wear of the joint cartilaginous surfaces of the hip. This gradually leads to a painful disability of the hip and the limb in concern. Some risk factors are found: heredity, deformities or misalignment of the lower limbs,obesity, rheumatic disease, osteonecrosis of the femoral head, and trauma history .The technical evolution of prosthetic surgery, mastering the postoperative and technical progress of the materials used made it possible to secure and make reliable the surgical treatment which is almost exclusively the fitting of a prosthesis.
DIAGNOSTIC
- Pain: main symptom : persistent, progressing by thrust at the beginning, of variable intensit,y becoming unbearable during crises, increasing during prolonged efforts.
- Stiffness: motion limitation is seen in advanced osteoarthritis
- Effusions concurrent thrusts, increasing pain which causes functional disability .
- Complementary examinations:
- Standard radiographs: are often sufficient to assess the importance of the joint space narrowing and the evolution of osteoarthritis stage.
- Telemetric radiographs: made in some particular case to calculate the axial deviations or inequality of the lower limbs length.
- MRI: very rare: in cases of unsophisticated osteonecrosis
TREATMENT
- Medical: Analgesics , anti-inflammatories, chondroprotectors , infiltrations (rarely with extreme caution ) , rehabilitation are used for first stages and can relieve pain without stopping osteoarthritis development.
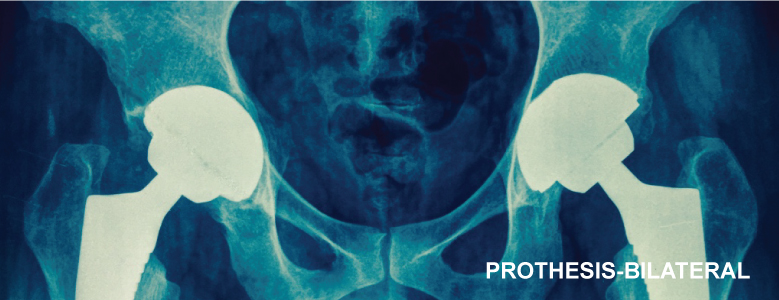
- Chirurgical: TOTAL HIP PROSTHESIS: THR.
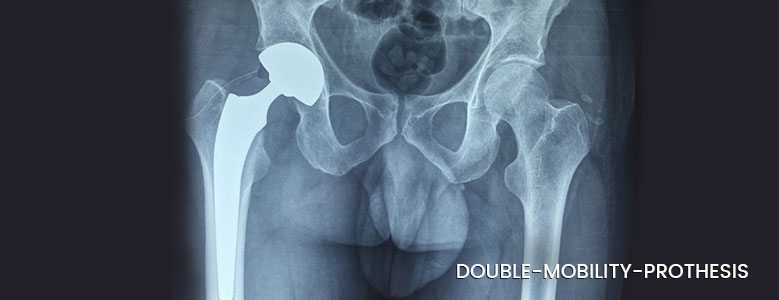
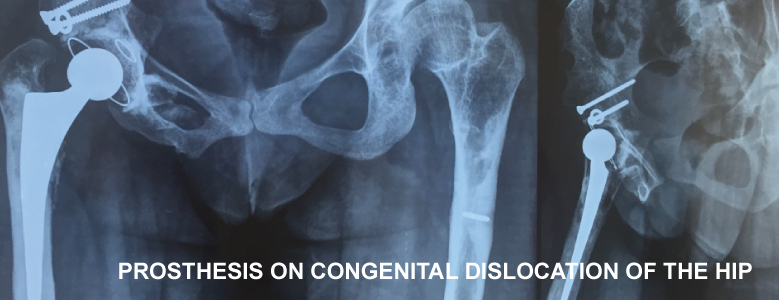
The decision will be based on the importance of osteoarthritis, discomfort sensation, patient’s will, his age and general health condition. The surgery should not be delayed if the patient’s autonomy tends to be reduced. The operation performed is a replacement of the joint surfaces with prosthetic parts. If this issue is unanimous, the type of prosthesis may vary. Indeed prostheses differ in their mode of anchorage (cemented or not), their materials (metal, titanium, polyethylene, ceramic), their primary stability (single, retentive, double mobility). Each type of prosthesis has its advantages and " drawbacks ", we believe that the choice is determined on a case by case basis depending of the patient himself ,which allows to optimize the results.
FOLLOW-UP
Hospitalizations average is 3-7 days..
Rehabilitation is immediate. The motion is activo-passive from the beginning (arthromoteur + + +). The support is immediate in the majority of cases. Particular attention is paid to prevent against the luxating postures.
Recovery is rapidly progressive with an almost normal movement within 1 month postoperative. Progression may take 6 months leaving an important margin of appreciation. The major short-and medium-term risk is the dislocation which ranges between 1and 3%. The emergency consultation of your surgeon is required.
Like any prosthesis ,this one has an average lifespan of 15 years. Regular follow-up is necessary in order to act in time in case of resumption necessity.