
PATHOLOGIES








Ruptures of the anterior cruciate ligament
The knee cruciate ligaments are two: anterior and posterior. These two elements are essential for the knee stability.
the anterior cruciate ligament rupture (ACL) is the most common in serious sprains of the knee. It occurs mostly for active persons due to quite intensive trauma: sports injuries (sudden knee twisting), work accident, road accident ...
DIAGNOSTIC
In the acute phase (immediately after injury):
- Pain: acute, intense when trauma
- creaking sensation sometimes audible inside the knee
- immediate appearance of large effusion at knee level
- functional disability and inability to continue activity
- Painful movement
- at this stage the ligament testing is quite difficult
At the chronicle phase:
- instability, with frequent episodes of knee derobements which is not reliable or sure
- difficulty of sport practicing at the same level
- Pain is uncommon and is not a characteristic feature of this phase,it may reflect a related meniscal lesion or the beginning of cartilaginous lesions for very old ruptures
- clinical examination is very specific and allows to diagnose almost surely through the ligament testing That finds an important drawer and / or a projection
paraclinical examination:
Radiographs: still practiced to eliminate fracture, osteoarthritis
MRI: best examination must be requested in case of any doubt => allows confirmation of the diagnosis and show potential related meniscal lesions
TREATMENT
- Médical: rehabilitation, essential element of treatment, pre-and postoperative. Some less active patients who do not wish to undergo surgery follow a specific program for three months to minimize the risk of instability..
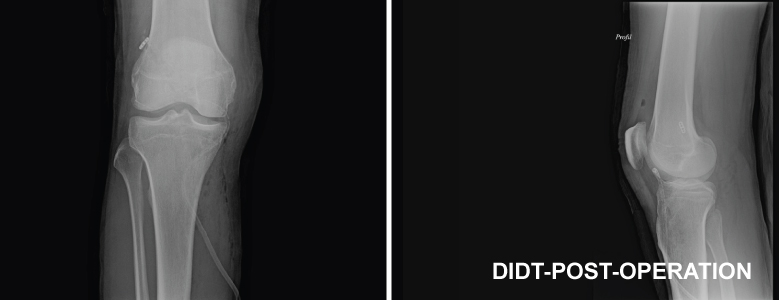
- Chirurgical: ACL graft performed in ARTHROSCOPY:
The cruciate ligaments lesions surgery has become a very reliable and minimally invasive operation thanks to this technique. It provides excellent results with very few complications. This technique consists of grafting the diseased cruciate ligament by replacing it with tendons taken from the same patient's knee (the middle part of the patellar tendon and half tendon).
This graft will be introduced into the knee reproducing the route and the function of the ACL through bone tunnels from both sides (in the tibia and the femur). This allows a natural integration of the graft.
Arthroscopy makes it possible to make this technique with minimally invasive manner (scar 3 to 5 cm) and very uneventful postoperative.
FOLLOW-UP
Hospitalizations average is 2-3 days.
Rehabilitation is immediate with an authorized support from the first day. It continues consistently for 6 months date from which the resumption of previous sporting activities may be considered.